Today’s Tip: Hypercholesterolemia and Hyperlipidemia
 Providers often use the terms hyperlipidemia and hypercholesterolemia interchangeably. Technically, hyperlipidemia is a high or elevated lipid/fat level in the blood. High blood cholesterol is a lipid disorder. As a result, when hyperlipidemia and hypercholesterolemia are both documented in the record, only assign code E78.00 (Pure hypercholesterolemia) per Coding Clinic, Second Quarter 2022. On the other hand, when ‘mixed hyperlipidemia’ and ‘hypercholesterolemia’ are both documented, assign code E78.2 (Mixed hyperlipidemia). In this example, hypercholesterolemia is included in the E78.2 code.
Providers often use the terms hyperlipidemia and hypercholesterolemia interchangeably. Technically, hyperlipidemia is a high or elevated lipid/fat level in the blood. High blood cholesterol is a lipid disorder. As a result, when hyperlipidemia and hypercholesterolemia are both documented in the record, only assign code E78.00 (Pure hypercholesterolemia) per Coding Clinic, Second Quarter 2022. On the other hand, when ‘mixed hyperlipidemia’ and ‘hypercholesterolemia’ are both documented, assign code E78.2 (Mixed hyperlipidemia). In this example, hypercholesterolemia is included in the E78.2 code.
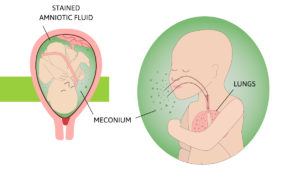 Meconium gives the amniotic fluid a greenish color. This is called meconium staining. Coding Clinic, Second Quarter 2022 clarifies ‘light meconium-stained fluid’ and how to code it. The presence of any meconium staining may indicate fetal distress, therefore code O77.0 (Labor and delivery affected by meconium in amniotic fluid) is appropriate to code if documented as such. There does not need to be documentation of fetal distress or maternal conditions to code.
Meconium gives the amniotic fluid a greenish color. This is called meconium staining. Coding Clinic, Second Quarter 2022 clarifies ‘light meconium-stained fluid’ and how to code it. The presence of any meconium staining may indicate fetal distress, therefore code O77.0 (Labor and delivery affected by meconium in amniotic fluid) is appropriate to code if documented as such. There does not need to be documentation of fetal distress or maternal conditions to code.
2022 ICD-10-CM CODE O77.0
 Eliquis can be used as an anticoagulant or an antithrombotic. When a patient is on Eliquis long-term, it can be a coding conundrum. As published in Coding Clinic, Second Quarter 2022, ICD-10-CM classifies Eliquis as an anticoagulant medication. Therefore, if long-term use of Eliquis is documented in the record, assign code Z79.01 (The long-term (current) use of anticoagulants).
Eliquis can be used as an anticoagulant or an antithrombotic. When a patient is on Eliquis long-term, it can be a coding conundrum. As published in Coding Clinic, Second Quarter 2022, ICD-10-CM classifies Eliquis as an anticoagulant medication. Therefore, if long-term use of Eliquis is documented in the record, assign code Z79.01 (The long-term (current) use of anticoagulants).
 This condition is commonly documented along with chronic kidney disease (CKD). MBD is a broad term used to describe a group of bone disorders of bone strength usually caused by mineral abnormalities such as calcium, phosphorus, vitamin D, or magnesium. As published in Coding Clinic, Second Quarter 2022, when MBD is a component of another disease process, only the underlying condition (e.g., secondary hyperparathyroidism or renal osteodystrophy) is coded. If no underlying condition is documented, code the appropriate code from subcategory M89.8X-.
This condition is commonly documented along with chronic kidney disease (CKD). MBD is a broad term used to describe a group of bone disorders of bone strength usually caused by mineral abnormalities such as calcium, phosphorus, vitamin D, or magnesium. As published in Coding Clinic, Second Quarter 2022, when MBD is a component of another disease process, only the underlying condition (e.g., secondary hyperparathyroidism or renal osteodystrophy) is coded. If no underlying condition is documented, code the appropriate code from subcategory M89.8X-.
 When Lupus (unspecified) is documented in a record, there is no default code. Therefore, it is important to have providers document this condition as precisely as possible.
When Lupus (unspecified) is documented in a record, there is no default code. Therefore, it is important to have providers document this condition as precisely as possible.
For instance, document SLE (systemic lupus erythematosus) instead and add any complications that accompany this diagnosis. It is often accompanied by Sjogren’s syndrome or Sicca syndrome, which have very specific codes. Another solution is to develop facility or provider-specific guidelines to report M32.9 (SLE, unspecified) as a default for Lupus, unspecified.
 Drug-induced neuropathy (D62.0) is a diagnosis often missed by even the savviest and seasoned coders. It is sometimes seen in documentation as ‘CIPN’ (chemotherapy-induced peripheral neuropathy) and is a common side effect caused by antineoplastic agents. Treatment includes steroids and nerve pain medication such as Gabapentin.
Drug-induced neuropathy (D62.0) is a diagnosis often missed by even the savviest and seasoned coders. It is sometimes seen in documentation as ‘CIPN’ (chemotherapy-induced peripheral neuropathy) and is a common side effect caused by antineoplastic agents. Treatment includes steroids and nerve pain medication such as Gabapentin.
Drugs related to neuropathy
The most likely chemotherapy drugs related to neuropathy include platinum drugs, such as oxaliplatin; taxanes, such as docetaxel; vinca alkaloids, such as vincristine; and myeloma treatments, such as bortezomib. This code can also be accompanied by another code for the adverse effect (T36-T50) to identify the drug.
 Cachexia (R64) is also known as ‘wasting’ or ‘wasting syndrome’. It is a general state of weakness involving marked weight and muscle loss. Emaciated is another term that may be found in the documentation that also maps to code R64.
Cachexia (R64) is also known as ‘wasting’ or ‘wasting syndrome’. It is a general state of weakness involving marked weight and muscle loss. Emaciated is another term that may be found in the documentation that also maps to code R64.
These diagnoses are often missed since they are commonly only seen in the Physical Exam or Review of Systems portion of a record. There are often ‘knee-jerk’ reactions that can lead a coder to investigate further if a patient may have these diagnoses.
What to look for
Cachexia is commonly seen in patients who have AIDS, cancer, or other advanced heart or lung disease. You will often see a lack of appetite, fatigue, low BMI, and malnutrition. Look for nutritional consults and a PEG tube in the documentation to trigger the search for cachexia in the documentation.
Why is this so important?
Cachexia is a diagnosis that can affect reimbursement for both Inpatient and Risk Adjustment. Don’t miss it!
Jeanie Heck, our Director of Education, begins our 2022 series of E/M Hot Topics with a discussion on Telemedicine. January’s Hot Topic provides an update from the CMS Final Rule as well as some reliable and reputable sources of information regarding telehealth.
For additional information about E/M Guideline Updates education, contact us.
Follow us on LinkedIn to keep up-to-date.
Jeanie Heck, our Director of Education, wraps up our E/M Hot Topic series for 2021 discussing the new 2022 Principal Care Management Services codes. In 2022, we will have three general categories of Care Management in our E/M section. The new PCM codes allow providers, qualified health care practitioners, and clinical staff to report a code(s) for the management of a single chronic condition.
For additional information about E/M Guideline Updates education, contact us.
Follow us on LinkedIn to keep up-to-date.
August 2021
In this month’s E/M Hot Topic, Jeanie Heck, our Director of Education, discusses “Drug Therapy Requiring Intensive Monitoring for Toxicity”. This falls under the HIGH level in our Risk element or level 5 (99205/99215). We now have a published definition for this in our 2021 CPT manual. This definition was further clarified by the CPT editorial panel in the Errata & Technical corrections document.
For additional information about E/M Guideline Updates education, contact us.
Follow us on LinkedIn to find out when the next E/M Hot Topic is released.
 “Here come the ‘chart police.’”
“Here come the ‘chart police.’”
 “Here come the ‘chart police.’”
“Here come the ‘chart police.’” Every clinical documentation specialist (CDS) has heard it. “Chart police.” For those CDSs with a nursing background, it is often heard from those nurses they have worked alongside in the following ways:
(1) when discussing their new role
(2) while explaining their current role
(3) when attempting to recruit bedside nurses into the CDS career path.
How do we educate our bedside-loving peers about the value that their documentation brings to the final coded record? Show them.
Nurses love evidence.
It has been the foundation of nursing practice since Florence Nightingale demonstrated that good hygiene improved outcomes. Pull up a stand-alone encoder and show them the difference made by inclusion of wound staging or body mass index. Clinical documentation integrity is an obscure role to most nurses so take the opportunity to translate the language. Instead of demonstrating the MS-DRG, show the difference in severity of illness (SOI) and risk of mortality (ROM) when including their documentation. Interpreting SOI and ROM is a quicker soap box discussion than CC/MCC capture and translates clinically with almost no discussion.
ICD-10-CM Guidelines for Coding and Reporting allow us “few exceptions” to the rule that “code assignment is based on the documentation by patient’s provider” but, nurses need to know that their documentation often triggers CDSs to know that a query opportunity exists. Default templates utilized by providers may repeatedly explain that the patient is oriented, but night shift nurse documentation may paint a different picture of a sundowning patient. That picture is incredibly valuable to the accuracy of the coded record, particularly when the provider is documenting in progress notes when assessing the same patient during the day.
The remote world has done wonders for production but can put a strain on those opportunities to engage our healthcare partners and demonstrate value. Other ways to engage our nursing colleagues in understanding the value of their education: round with them during an onsite day, engage nursing management to become part of the nursing skills fairs (quality documentation is inarguably a skill), or seek out the opportunity to present to new nursing hires during orientation.
July 2021
In July’s E/M Hot Topic, Jeanie Heck, our Director of Education, discusses the new guidelines for Time and the Prolonged Time codes. The new 2021 E/M guidelines are significantly different from the way we previously used to account for Time. She also addresses the latest technical corrections regarding Time from the AMA’s webinar at the end of May and gives some documentation template examples to help educate your providers.
For additional information about E/M Guideline Updates education, contact us.
Follow us on LinkedIn to find out when the next E/M Hot Topic is released.